
Hand Anatomy: Bones, Nerves & Muscles Guide (Canada)
Share
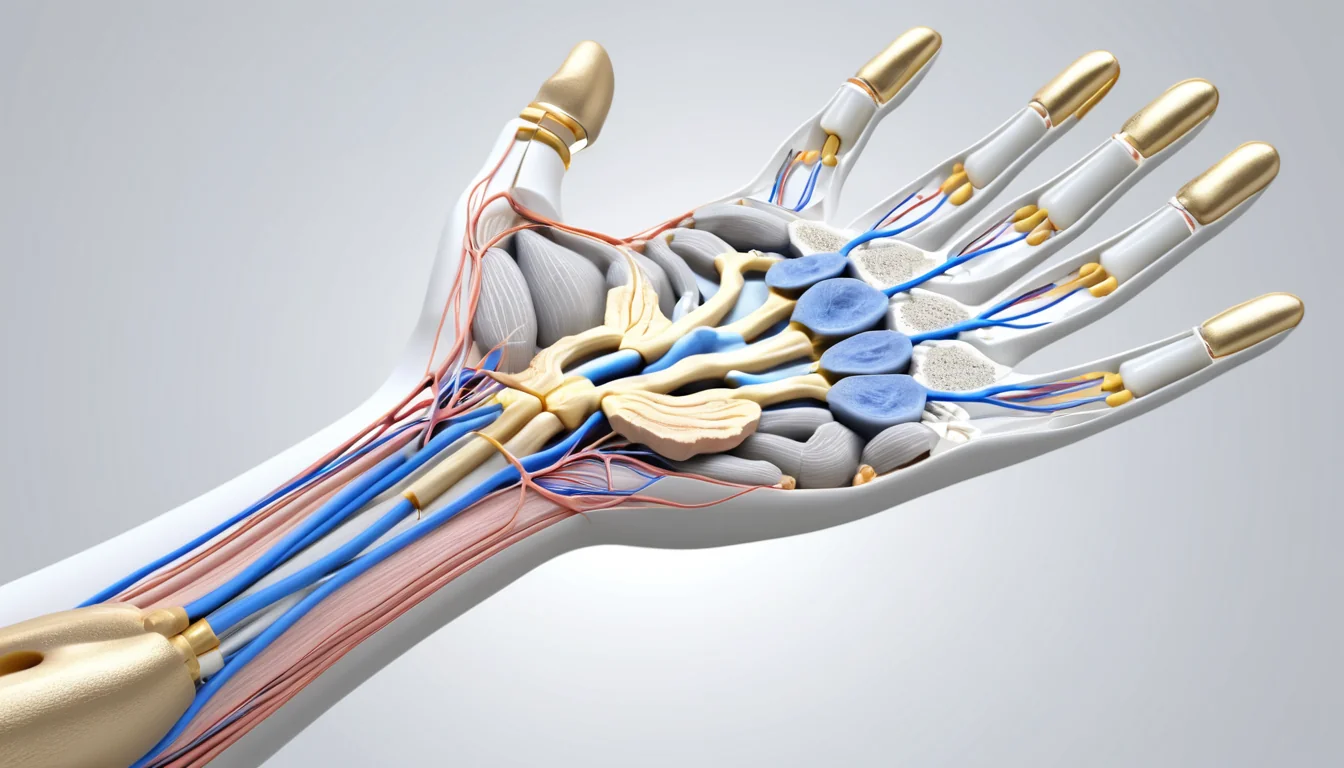
Hand anatomy is one of the most complex and remarkable systems in the human body, with 27 bones, dozens of muscles, three major nerves, and layers of specialized skin all working together to give you incredible grip, sensation, and precision. Whether you are a Canadian healthcare student, someone recovering from an injury, or simply curious about how your body works, understanding the structure of your hand can help you recognize problems early and make informed decisions about your health.
Understanding Your Hand Anatomy: Bones, Nerves, and Skin
This comprehensive guide breaks down every major component, from the carpal bones of your wrist to the nerves that control feeling and movement. We explain the bones of the hand, the unique properties of palm and dorsal skin, the deep compartments of the palm, and the nerve pathways that make your hand one of the most sensitive parts of your body. Written in plain language for Canadian readers, this resource will help you understand what is happening beneath the surface and when it might be time to seek medical attention.
The Bones of the Hand: Your Hand Anatomy Foundation
| Structure Type | Key Components | Primary Function | Common Conditions |
|---|---|---|---|
| Bones | 27 bones including carpals, metacarpals, and phalanges | Provide structural framework, support grip and fine motor movements | Fractures, osteoarthritis, osteoporosis-related breaks |
| Nerves | Median, ulnar, and radial nerves | Transmit sensory signals and control muscle movement throughout the hand | Carpal tunnel syndrome, cubital tunnel syndrome, peripheral neuropathy |
| Tendons & Ligaments | Flexor and extensor tendons, collateral ligaments | Connect muscles to bones and stabilize joints during movement | Tendonitis, tendon tears, ligament sprains |
| Skin & Soft Tissue | Dermis, epidermis, subcutaneous fat, fascia | Protect underlying structures, provide sensation and grip friction | Dupuytren’s contracture, cellulitis, contact dermatitis |
| Blood Vessels | Radial and ulnar arteries, palmar arches, digital arteries | Deliver oxygen and nutrients to hand tissues and support wound healing | Raynaud’s phenomenon, arterial insufficiency, vascular injury |
The skeleton of the hand and wrist contains 27 bones in total. These bones fall into three main groups: the carpal bones, the metacarpals, and the phalanges. Each group plays a specific role in how your hand moves and functions.
Carpal Bones: The Wrist Complex
The wrist is the most complex joint in the human body. It is made up of eight carpal bones arranged in two rows. The top row (proximal row), running from the thumb side to the pinky side, includes the scaphoid, lunate, triquetrum, and pisiform. The bottom row (distal row) contains the trapezium, trapezoid, capitate, and hamate.
Most of these bones work together to move the wrist. However, the pisiform is a sesamoid bone — a bone embedded within a tendon — and it does not directly take part in wrist movement. The scaphoid bone connects both rows, which makes it the most vulnerable carpal bone to fracture during a fall.
The distal row of carpal bones is firmly attached to the second and third metacarpals. Together, they form a fixed unit. All other structures in the hand move in relation to this stable base. This is important to understand when treating wrist and hand injuries.
Metacarpal Bones: The Palm of Your Hand
The palm of your hand contains five metacarpal bones. Each metacarpal has a base, a shaft, a neck, and a head. The first metacarpal — the one connected to your thumb — is the shortest and most mobile. It connects to the trapezium bone of the wrist.
The other four metacarpals connect to the trapezoid, capitate, and hamate bones at their bases. At their other end, each metacarpal head connects to the first bone of each finger. This joint is what allows your fingers to bend and straighten.
Phalanges: The Finger Bones
Your hand contains 14 phalanges, which are the bones that make up your fingers. Each finger has three phalanges: a proximal phalanx (closest to the palm), a middle phalanx, and a distal phalanx (the fingertip). The thumb is the only digit with just two phalanges — a proximal and a distal.
To avoid confusion, fingers are named by position: thumb (also called the pollex), index, middle, ring, and little finger. Understanding how wrist and hand fractures occur is easier when you know these bone names.
Hand Skin: Two Very Different Surfaces
The skin on your hand is not the same on both sides. The back of the hand and the palm each have unique structures suited to their specific jobs. This difference has real clinical importance for surgeons and family doctors alike.
The Back of the Hand
The skin on the back (dorsal surface) of the hand is thin and flexible. It sits loosely over the skeleton, connected by soft, open connective tissue that contains veins and lymphatic vessels. Because of this loose attachment, swelling tends to appear on the back of the hand first — even when the injury is on the palm side.
This loose connection also makes the skin on the back of the hand more vulnerable to injury. It can blister more easily and is more likely to be damaged in a traumatic injury. In addition, surgeons must consider this when planning incisions in this area.
The Palm of the Hand
Palm skin is thick, tough, and firmly anchored. It connects to a layer of tissue beneath it called the subcutaneous fascia through many vertical fibres. This firm attachment is what allows your hand to grip objects without the skin sliding around.
The palm is also richly supplied with blood through small vertical branches from the digital arteries. As a result, blisters form much less easily on the palm than on the back of the hand. Furthermore, the palmar skin contains a very high number of sensory receptors. These tiny nerve endings are essential for touch, temperature, and pressure — the fine sensations that make your hand so useful in daily life.
Fingernails and Their Role in Hand Anatomy
Fingernails are specialized structures that grow from the skin. They develop from a germinal matrix — a layer of tissue at the base of the last finger bone (distal phalanx). The part of the nail matrix beyond the white crescent (lunula) is called the sterile matrix. It has a rich blood supply, which gives it a pink colour.
The entire nail matrix sits in very close contact with the bone beneath it. Therefore, a fracture of the distal phalanx can easily damage the nail matrix. This is why fingertip injuries often affect nail growth long after the initial injury heals.
Palmar Fascia and the Deep Compartments
Beneath the palm skin lies a tough layer of fibrous tissue called the palmar fascia. This layer is made up of fibres running in multiple directions: longitudinal (lengthwise), transverse (across), oblique (diagonal), and vertical (up and down).
The longitudinal fibres start at the wrist — specifically from the palmaris longus tendon, when it is present (some people are born without this tendon) — and extend toward the base of each finger. Along the way, smaller fibres branch off and anchor to surrounding tissue. Together, these fibres form the fibrous flexor system for each finger.
Deep Compartments of the Palm
The vertical fibres of the palmar fascia connect to the skin above and the metacarpal bones below. This arrangement creates eight separate compartments within the palm. Each compartment holds the flexor tendons and the neurovascular bundle (nerve and blood vessel package) for one finger. A shared central compartment sits at the base of the palm.
Two important fascial bands run along each finger: Grayson’s ligament (on the palm side) and Cleland’s ligament (on the back side). These ligaments sit on either side of the finger’s neurovascular bundle. Surgeons must know this anatomy precisely during procedures like palmar fasciectomy — a surgery used to treat Dupuytren’s contracture, a condition where the palm tissue tightens and pulls fingers into a bent position. You can learn more about this condition from Healthline’s overview of Dupuytren’s contracture.
The Nerves of the Hand
Three major nerves control sensation and movement in the hand: the median nerve, the ulnar nerve, and the radial nerve. Each nerve carries both motor signals (telling muscles to move) and sensory signals (sending touch information to the brain). In many people, the exact distribution of these nerves varies slightly — so what textbooks show as the “classic” pattern is really just a common starting point.
The Median Nerve
The median nerve is responsible for the fine movements and grip function of the hand. It originates from the brachial plexus — a network of nerves in the neck and shoulder — from nerve roots C5 through T1. In the forearm, it sends motor branches to the muscles that pronate the forearm and flex the wrist.
The median nerve is the nerve affected in carpal tunnel syndrome, one of the most common hand conditions seen in Canadian walk-in clinics and family doctor offices. When this nerve is compressed at the wrist, people experience numbness, tingling, and weakness in the hand. Health Canada recognizes repetitive strain injuries, including carpal tunnel syndrome, as a significant workplace health concern.
The Ulnar and Radial Nerves
The ulnar nerve controls the small muscles of the hand and provides sensation to the little finger and the inner half of the ring finger. Injury to this nerve — often from leaning on the elbow for long periods — causes a condition sometimes called “cubital tunnel syndrome.”
The radial nerve mainly controls the muscles that extend the wrist and fingers. It provides sensation to the back of the hand on the thumb side. Damage to the radial nerve can result in “wrist drop,” where a person cannot lift their wrist or straighten their fingers.
When to See a Doctor About Hand Pain or Injury
Hand problems are very common and can affect people of all ages. If you experience any of the following, it is important to seek medical advice promptly. Your family doctor is a great first point of contact, and most provincial health plans in Canada cover assessment and referral for hand conditions.
- Sudden severe pain after a fall — this could indicate a fracture, especially of the scaphoid bone
- Numbness or tingling in the fingers — this may signal nerve compression such as carpal tunnel syndrome
- Swelling that does not go down within 48 hours — persistent swelling warrants evaluation
- Loss of grip strength — weakness can point to nerve or tendon damage
- Fingers that are bent and cannot straighten — this could be a sign of Dupuytren’s contracture or a tendon injury
- Nail changes after a fingertip injury — nail matrix damage may need specialist care
If your family doctor is not immediately available, a walk-in clinic can assess most hand injuries and arrange X-rays if needed. For severe injuries — such as an open fracture, deep cut, or suspected tendon rupture — go to your nearest emergency department right away. Always consult a qualified healthcare provider before starting any treatment for a hand condition.
What are the 27 bones of the hand called?
The 27 bones in hand anatomy are divided into three groups: 8 carpal bones in the wrist, 5 metacarpal bones in the palm, and 14 phalanges in the fingers. Understanding these bones is important for diagnosing fractures and other hand injuries. Your family doctor or a radiologist can identify them on an X-ray.
Which bone in the hand breaks most often?
The scaphoid is the most commonly fractured carpal bone in hand anatomy, often broken during a fall on an outstretched hand. It is vulnerable because it bridges both rows of wrist bones. Scaphoid fractures can be tricky to spot on X-ray, so your doctor may order an MRI if they suspect this injury.
What nerve is affected by carpal tunnel syndrome?
Carpal tunnel syndrome affects the median nerve, one of the three main nerves in hand anatomy. When this nerve is compressed at the wrist, it causes numbness, tingling, and weakness in the thumb, index, middle, and part of the ring finger. A family doctor or walk-in clinic can assess symptoms and refer you to a specialist if needed.
Why does the back of the hand swell more than the palm after an injury?
This comes down to hand anatomy: the skin on the back of the hand is loosely attached to the underlying skeleton, giving fluid room to collect there. The palm skin, by contrast, is firmly anchored by vertical fibres, which limits swelling on that side. This is why swelling often appears on the back of the hand even when the injury is on the palm.
What is Dupuytren’s contracture and how does hand anatomy explain it?
Dupuytren’s contracture is a condition where the palmar fascia — a layer of fibrous tissue in hand anatomy — thickens and tightens over time. This pulls one or more fingers into a bent position that cannot be straightened. Treatment often involves surgery to release or remove the affected tissue, which requires detailed knowledge of the hand’s fascial compartments and nerves.
How many phalanges does the thumb have compared to other fingers?
According to Mayo Clinic’s guide to carpal tunnel syndrome, this information is supported by current medical research.
For more information, read our guide on understanding your white blood cell count results.
In hand anatomy, the thumb has only two phalanges — a proximal and a distal — while every other finger has three (proximal, middle, and distal). This is one reason the thumb moves differently and has greater range of motion than the other fingers. The thumb’s unique structure makes it essential for gripping and fine motor tasks.
Key Takeaways
- Hand anatomy involves 27 bones grouped into carpal bones, metacarpals, and phalanges.
- The scaphoid bone is the most vulnerable to fracture because it connects both rows of wrist bones.
- The skin on the back of the hand is loose and flexible; palm skin is thick and firmly anchored for gripping.
- The palm contains a rich network of sensory receptors essential for touch and fine movement.
- Three major nerves — median, ulnar, and radial — control both sensation and movement in the hand.
- The palmar fascia creates compartments that protect tendons and nerves; its thickening causes Dupuytren’s contracture.
- Hand pain, numbness, or swelling that persists should be assessed by your family doctor or walk-in clinic.
- Most hand conditions are covered under provincial health plans in Canada — do not delay seeking care.
Frequently Asked Questions
What is hand anatomy made up of?
Hand anatomy consists of 27 bones, including carpals, metacarpals, and phalanges, along with muscles, tendons, ligaments, nerves, and blood vessels. The skin provides protective covering, while three major nerves — median, ulnar, and radial — control sensation and movement throughout the hand and fingers.
What are the symptoms of hand nerve damage?
Symptoms of hand nerve damage include numbness, tingling, burning sensations, muscle weakness, and loss of grip strength. You may also experience sharp shooting pain or difficulty performing fine motor tasks like buttoning clothing. Symptoms vary depending on which nerve — median, ulnar, or radial — is affected.
How is a hand injury treated in Canada?
Hand injury treatment in Canada depends on severity. Minor injuries involve rest, ice, compression, and elevation (RICE). Fractures may require splinting or casting. Tendon or nerve damage often needs surgical repair followed by physiotherapy. Most Canadians access initial care through walk-in clinics or emergency departments before specialist referral.
How can you prevent hand anatomy injuries at work?
Prevent hand injuries at work by wearing appropriate protective gloves, using ergonomic tools, taking regular breaks to reduce repetitive strain, and following workplace safety protocols. Stretching exercises, proper lifting techniques, and maintaining good posture also significantly reduce the risk of tendon, nerve, and joint injuries.
When should I see a doctor about hand anatomy pain?
See a doctor if hand pain is severe, persistent beyond a few days, accompanied by swelling, visible deformity, numbness, or significant weakness. Seek immediate emergency care for open wounds, suspected fractures, or complete loss of sensation. Early diagnosis prevents long-term damage to bones, nerves, and tendons.
About the Author
Dr. Sarah Mitchell, MDDr. Sarah Mitchell is a board-certified family physician with over 15 years of clinical experience. She completed her MD at the University of Toronto and her residency at Toronto General Hospital. Dr. Mitchell specializes in preventive medicine and chronic disease management. She is a member of the College of Family Physicians of Canada (CFPC) and has published over 30 peer-reviewed articles on preventive health care.
View all articles →

{kind=link}