
Rheumatoid Foot: Symptoms, Deformities & Treatment Canada
Share
Rheumatoid foot is a painful and progressive condition that affects thousands of Canadians living with rheumatoid arthritis, causing significant joint damage, deformity, and loss of mobility. When the immune system attacks the joints of the feet, everyday activities like walking and wearing shoes become increasingly difficult — making early recognition essential for preserving quality of life.
Understanding the Rheumatoid Foot: What Makes It Unique
Understanding the symptoms of rheumatoid arthritis feet problems can help you take action before irreversible damage occurs. In Canada, where access to rheumatologists and specialized foot care varies by province, knowing what to look for and when to seek help is critical. This guide covers the causes, common deformities, diagnostic approaches, and treatment options available to Canadians dealing with this challenging condition.
What Is Rheumatoid Foot?
| Deformity Type | Characteristics | Common Location | Management Approach |
|---|---|---|---|
| Hallux Valgus (Bunion) | Lateral deviation of the big toe with bony prominence at the first metatarsophalangeal joint; pain and swelling common | First MTP joint | Wider footwear, custom orthotics, splinting; surgical correction in severe cases |
| Hammer Toe | Abnormal flexion contracture of the proximal interphalangeal joint causing a downward curl; may develop painful corns | Second to fifth toes | Toe pads, custom orthotics, physical therapy; surgical straightening if conservative measures fail |
| Claw Toe | Hyperextension at MTP joint combined with flexion at both interphalangeal joints; often causes calluses and ulceration risk | Lesser toes | Accommodative footwear, metatarsal pads, wound care if ulceration present; surgical correction considered |
| Pes Planus (Flat Foot) | Progressive collapse of the medial longitudinal arch due to posterior tibial tendon dysfunction and ligament laxity | Midfoot and hindfoot | Arch-support orthotics, ankle-foot orthoses (AFOs), physiotherapy; hindfoot fusion surgery in advanced cases |
| Metatarsalgia | Inflammation and pain beneath the metatarsal heads due to synovitis and fat pad displacement; worsens with weight-bearing | Forefoot/metatarsal heads | Metatarsal padding, cushioned insoles, activity modification, NSAIDs or corticosteroid injections as prescribed |
The foot is the part of your lower limb that sits below the ankle. A rheumatoid foot is a foot that has been damaged and deformed by rheumatoid arthritis (RA). RA is a chronic inflammatory disease that attacks your joints and can also affect your internal organs.
RA is not just “wear and tear” arthritis. It is an autoimmune condition, meaning your immune system mistakenly attacks healthy tissue. Over time, this causes joint destruction, loss of function, and significant changes to the shape of your feet. You can learn more about rheumatoid arthritis from Mayo Clinic’s overview of rheumatoid arthritis.
How Rheumatoid Arthritis Affects Your Joints
Joint involvement in RA starts early and progresses steadily. It typically appears in a symmetrical pattern — meaning both sides of the body are affected at the same time. Pain and swelling are most common in the hands, wrists, and the front part of the foot (called the forefoot).
Research shows that X-ray changes in the forefoot appear in up to 69% of patients within the first three months of the disease. Interestingly, the feet are affected twice as often as the hands.
Which Joints Are Affected?
RA attacks joints in a specific order. The most commonly affected joints, from most to least frequent, include:
- The metatarsophalangeal joints (the knuckles of your feet, where your toes meet the foot)
- The knuckles of your hands
- The wrist bones
- The proximal interphalangeal joints (the middle knuckles of your toes)
- The bones of the wrist and hand (the carpus)
- The big toe joint
As the disease progresses, larger joints like the shoulder, elbow, hip, knee, and ankle are also commonly involved. In addition, a serious — and potentially life-threatening — complication called atlantoaxial subluxation can occur. This is an instability between the top two vertebrae in your neck, and it requires urgent medical attention.
Symptoms Beyond the Joints
RA is a whole-body disease. It does not only affect your joints. Many Canadians with RA experience symptoms in other parts of the body as well.
Skin and Circulation
Common skin-related symptoms include rheumatoid nodules (firm lumps under the skin), dry eyes and dry mouth (a sign of a related condition called Sjögren’s syndrome), and Raynaud’s phenomenon — where fingers or toes turn white or blue in the cold.
Lungs and Heart
RA can cause fluid around the lungs (pleurisy) and inflammation around the heart (pericarditis). These complications may develop without obvious symptoms, so regular check-ups with your family doctor are important.
Kidneys and Nerves
Long-term RA or its treatments can affect kidney function. Nerve-related complications include carpal tunnel syndrome and, in more serious cases, compression of the spinal cord due to cervical spine instability. If you notice weakness or sores on your lower legs, this could signal a serious complication called rheumatoid vasculitis. This requires urgent treatment to prevent lasting damage.
For a broader look at how systemic inflammation affects the body, the World Health Organization’s fact sheet on chronic rheumatic conditions provides helpful context.
The Rheumatoid Foot: What Makes It Unique
The rheumatoid foot has several features that set it apart from other foot problems. The forefoot is affected in roughly 70 to 90 percent of people with RA. This causes significant pain and functional loss — and the changes can happen very quickly.
Rapid Deformity
One of the most striking features of the rheumatoid foot is how fast deformities appear. Bunion-like bumps and bent-toe deformities (called “claw toes” or “hammer toes”) can develop in as little as six months. However, these are not the same as ordinary bunions. They represent a different underlying process caused by RA itself.
Many patients find it increasingly hard to fit into regular shoes. Walking normally becomes a challenge. These changes often appear on both feet, but they may not look the same on each side — one foot may be worse than the other, or the deformity may take a slightly different shape.
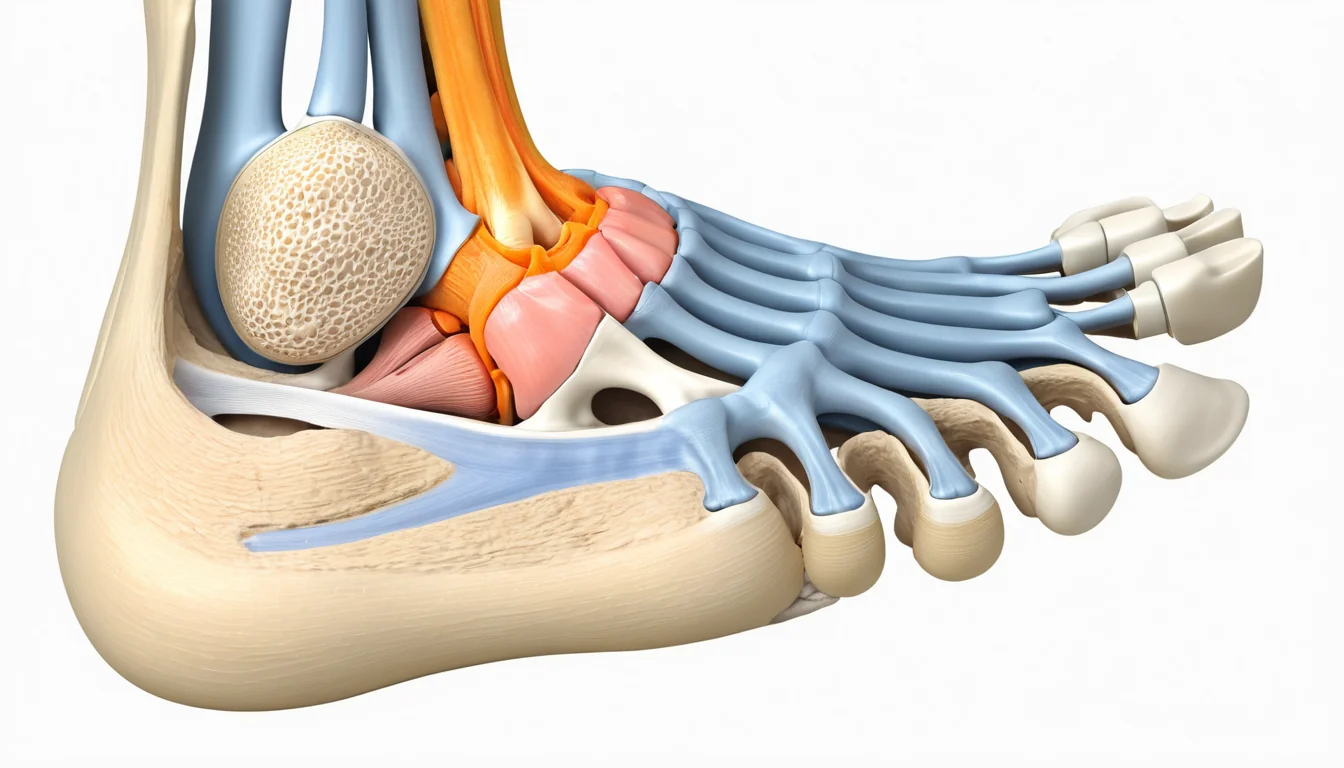
What Happens Inside the Foot
RA weakens several important structures in the forefoot at the same time. The joints, joint capsules, plantar plates (the tough tissue on the bottom of the foot), ligaments, and tendons all become inflamed and then damaged. Most of these structures normally work together to support the foot’s shape and function.
As these structures break down, the metatarsal bones (the long bones in the middle of your foot) begin to spread apart. The heads of these bones can start to push downward through the sole of the foot. This happens not because the arch “collapses” in the traditional sense, but because the plantar plate is destroyed and the small muscles of the foot lose their balance. As a result, the toe joints can dislocate.
The small muscles that normally keep your toes straight — called the interosseous and lumbrical muscles — stop working properly. This leads to secondary toe deformities, including “hammer toes” where the toes curl downward in a claw-like position. Furthermore, RA-related inflammation of the tendons (tenosynovitis) can cause tendons to weaken and eventually tear.
Types of Forefoot Deformity
Foot specialists classify rheumatoid forefoot deformities into several types:
- Triangular foot: The foot takes on a triangular shape as the toes splay out.
- Fibular deviation: The toes drift toward the outside of the foot (toward the little toe side).
- Tibial deviation: The toes drift toward the inside of the foot (toward the big toe side).
- “Windswept” toes: The toes deviate in multiple directions, giving a chaotic appearance.
How Doctors Evaluate the Rheumatoid Foot
A foot specialist — typically an orthopaedic surgeon or podiatrist — will assess the rheumatoid foot by focusing on three key questions.
1. What Does the Patient Need?
The specialist looks at how well your foot functions overall. They assess each joint individually, but they pay special attention to how your foot affects your daily activities — things like walking, climbing stairs, and fitting into footwear.
2. How Active Is the Disease?
RA is a fluctuating disease. It goes through flares (periods of high activity) and remissions (calmer periods). Specific blood tests and imaging can measure how active the disease is. Your foot specialist will work closely with your rheumatologist to time any treatments appropriately.
3. What Treatment Is Right for You?
Treatment aims to reduce pain and maintain function. Honest expectations are important here. In many cases, surgery for the rheumatoid foot is palliative — meaning it focuses on relieving pain and improving comfort rather than fully correcting the deformity. True reconstructive surgery is possible in some patients but is less common.
Non-surgical options include specially fitted orthotics, wide toe-box footwear, physiotherapy, and medications managed by your rheumatologist. The goal of modern RA drug therapy — including biologics and disease-modifying drugs — is to slow or stop joint destruction before serious foot deformity develops. Healthline’s guide to rheumatoid arthritis foot pain offers additional practical tips for managing symptoms at home.
When to See a Doctor
If you have been diagnosed with rheumatoid arthritis and you notice changes in your feet — such as pain in the ball of the foot, toes that are drifting or curling, or swelling around the toe joints — bring it up at your next appointment. Do not wait until the deformity becomes severe.
If you do not yet have a rheumatologist, start by visiting your family doctor or a walk-in clinic. Ask for a referral to a rheumatologist, and mention any foot pain specifically. Provincial health plans across Canada cover rheumatology consultations when referred by a primary care provider.
Seek urgent care immediately if you experience sudden weakness or numbness in your legs, or if you develop open sores or ulcers on your lower limbs. These can be signs of rheumatoid vasculitis or spinal cord compression — both of which are medical emergencies.
Always speak with your family doctor or a qualified healthcare provider before starting or changing any treatment for rheumatoid arthritis or foot problems. This article is for informational purposes only and does not replace professional medical advice.
Frequently Asked Questions About Rheumatoid Foot
What does a rheumatoid foot look like?
A rheumatoid foot often shows bunion-like bumps, curled or clawed toes, and a wide, splayed forefoot. The toes may drift sideways or in multiple directions, and the ball of the foot may appear swollen or have visible bony prominences pushing through the sole.
Is rheumatoid foot the same as a regular bunion?
No. Although a rheumatoid foot can look similar to a bunion, it is a different condition. Regular bunions develop slowly due to foot mechanics and footwear, while rheumatoid foot deformities are caused by joint inflammation and destruction from rheumatoid arthritis — and can appear within just a few months.
Can rheumatoid foot be treated without surgery?
Yes, many people manage rheumatoid foot symptoms successfully without surgery. Custom orthotics, wide-fitting shoes, physiotherapy, and medications prescribed by a rheumatologist can all help reduce pain and slow the progression of deformity. Surgery is considered when conservative treatments no longer provide adequate relief.
How quickly does rheumatoid foot deformity progress?
The rheumatoid foot can change rapidly — sometimes within six months of the onset of rheumatoid arthritis. Early joint damage on X-rays has been found in nearly 70% of patients within the first three months. This is why early diagnosis and treatment of RA is so important for protecting foot health.
Which joints in the foot are most affected by rheumatoid arthritis?
The metatarsophalangeal joints — the joints where your toes connect to the rest of your foot — are the most commonly affected by rheumatoid arthritis. The big toe joint and the middle knuckles of the toes are also frequently involved. These joints are responsible for the push-off motion when you walk, so damage there has a major impact on mobility.
Should I see a rheumatologist or a foot specialist for rheumatoid foot?
According to Mayo Clinic’s overview of rheumatoid arthritis, this information is supported by current medical research.
For more information, read our guide on anemia symptoms that can accompany autoimmune arthritis foot problems.
Ideally, both. A rheumatologist manages the underlying disease with medications to slow joint destruction, while a foot specialist — such as an orthopaedic surgeon or podiatrist — addresses the mechanical and structural problems of the rheumatoid foot. Your family doctor can coordinate referrals to both specialists through your provincial health plan.
Key Takeaways
- Rheumatoid foot is a serious complication of rheumatoid arthritis that affects 70–90% of people with the condition.
- Deformities can develop very quickly — sometimes within six months — and affect both feet, though often unevenly.
- RA damages the joints, tendons, ligaments, and muscles of the foot all at once, causing the foot to spread, toes to curl, and joints to dislocate.
- Rheumatoid foot is not the same as ordinary bunions, even though the two can look similar.
- RA is a whole-body disease. Serious complications — including heart, lung, kidney, and spinal cord involvement — require regular monitoring.
- Early treatment of RA is the best way to protect your feet. Ask your family doctor about a rheumatology referral if you have joint pain and foot changes.
- Seek urgent care for sudden leg weakness, numbness, or open sores on your lower limbs.
- Treatment options include custom orthotics, appropriate footwear, physiotherapy, medication, and in some cases surgery — always guided by your healthcare team.
Frequently Asked Questions
What is rheumatoid foot?
Rheumatoid foot refers to foot and ankle complications caused by rheumatoid arthritis (RA), an autoimmune disease that attacks joint tissue. Chronic inflammation damages bones, cartilage, tendons, and ligaments in the foot, leading to pain, swelling, and progressive structural deformities. It affects up to 90% of people living with RA.
What are the symptoms of rheumatoid foot?
Common rheumatoid foot symptoms include persistent joint pain, morning stiffness, swelling, warmth, and tenderness across the forefoot, midfoot, or ankle. Over time, patients may develop visible deformities such as bunions, hammertoes, claw toes, and collapsed arches, making walking increasingly difficult and painful.
How is rheumatoid foot treated in Canada?
Rheumatoid foot treatment typically combines disease-modifying medications (DMARDs), custom orthotics, physiotherapy, and supportive footwear. For severe deformities, surgical options such as joint fusion or arthroplasty may be recommended. A rheumatologist and podiatrist often work together to manage symptoms and slow joint damage progression.
Can rheumatoid arthritis foot deformities be prevented?
Early diagnosis and consistent treatment with DMARDs can significantly slow the progression of foot deformities. Wearing well-fitted, supportive footwear, using custom orthotics, maintaining a healthy weight, and attending regular rheumatology appointments all help reduce the risk and severity of deformities developing over time.
When should I see a doctor about foot pain from rheumatoid arthritis?
See a doctor promptly if you experience persistent foot or ankle pain, visible joint swelling, increasing stiffness lasting over 30 minutes in the morning, or noticeable changes in foot shape. Early intervention can prevent irreversible joint damage, preserve mobility, and significantly improve your long-term quality of life.
About the Author
Dr. James Okafor, MD, PhDDr. James Okafor holds an MD and PhD in Neurological Sciences from McGill University. With 12 years of experience in clinical neurology and mental health research, he has contributed to landmark studies on depression, anxiety, and cognitive health. Dr. Okafor is a Fellow of the Royal College of Physicians and Surgeons of Canada and serves on the editorial board of two peer-reviewed journals.
View all articles →

{kind=link}