
Placental Abruption: Causes, Symptoms & What to Do
Share
Placental abruption is a serious pregnancy complication where the placenta separates from the uterine wall before birth, affecting roughly 9 out of every 1,000 pregnancies in Canada. Because the placenta delivers oxygen and nutrients from mother to baby, this early separation can be life-threatening for both and requires immediate medical attention.
What Is Placental Abruption and Why Is It Dangerous?
Understanding the causes of placental abruption, recognizing the warning signs early, and knowing what to do can help protect you and your baby. This guide covers everything Canadian parents need to know — from risk factors and diagnosis to treatment options available across Canada’s healthcare system.
What Is Placental Abruption?
| Type | Characteristics | Symptoms | Management |
|---|---|---|---|
| Mild (Grade 1) | Less than 25% of placenta detached; minimal bleeding; fetal heart rate normal | Light vaginal bleeding; mild uterine tenderness; no signs of fetal distress | Hospitalization for monitoring; bed rest; possible early delivery if near term; corticosteroids if preterm |
| Moderate (Grade 2) | 25–50% of placenta detached; moderate concealed or visible bleeding; some fetal compromise | Moderate vaginal bleeding; persistent uterine contractions; fetal heart rate abnormalities | Immediate hospitalization; continuous fetal monitoring; IV fluids and blood products; likely emergency delivery |
| Severe (Grade 3) | More than 50% of placenta detached; significant hemorrhage; high risk of fetal death | Heavy bleeding or no visible bleeding; rigid, board-like uterus; maternal shock; fetal distress or stillbirth | Emergency caesarean section; blood transfusion; ICU care for mother; management of disseminated intravascular coagulation (DIC) |
| Concealed Abruption | Blood trapped behind placenta; no external bleeding despite significant internal hemorrhage | Severe abdominal or back pain; uterine rigidity; rapid maternal deterioration without visible bleeding | Urgent ultrasound and clinical assessment; emergency delivery; close monitoring for coagulopathy and maternal shock |
| Partial Abruption | Only a portion of the placental surface separates; pregnancy may continue with close monitoring | Intermittent spotting or bleeding; mild cramping; may be asymptomatic in early stages | Regular obstetric follow-up; modified activity; serial ultrasounds; delivery planning based on gestational age and fetal well-being |
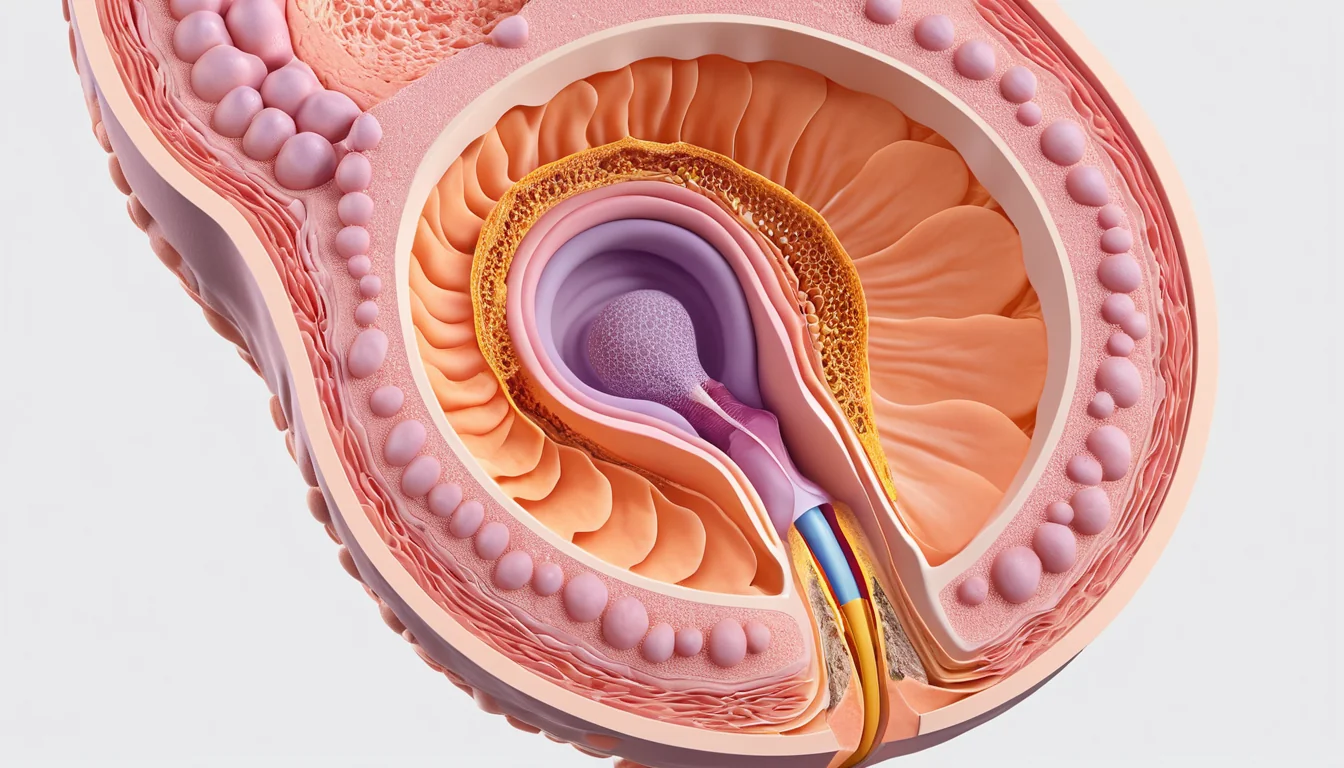
During a healthy pregnancy, the placenta stays firmly attached to the inner wall of the uterus until after the baby is born. With placental abruption, that attachment breaks down too early. The placenta peels away — partially or fully — before delivery.
This condition usually occurs in the third trimester. However, it can happen any time after week 20 of pregnancy. In some cases, up to 15% of abruptions are not detected until labour begins or after delivery.
Placental abruption can lead to premature birth, low birth weight (under 2,500 grams), and severe blood loss in the mother. In rare cases — fewer than 1 in 1,000 births — a severe abruption can result in the loss of the baby. This is why fast medical attention is so important.
Causes of Placental Abruption
Doctors do not fully understand what causes placental abruption in every case. Some women develop it with no clear explanation. However, researchers have identified several risk factors that are closely linked to the condition.
It is important to know that having a risk factor does not mean you will develop placental abruption. It simply means your risk may be higher than average. Talking openly with your healthcare provider helps you stay informed and prepared.
High Blood Pressure
High blood pressure — 140/90 mmHg or higher — is the most common risk factor linked to placental abruption. This includes chronic high blood pressure and pregnancy-induced high blood pressure, known as preeclampsia. Managing blood pressure throughout your pregnancy is one of the most important steps you can take.
Previous Placental Abruption
If you have had a placental abruption before, your risk of having another one is between 4% and 17%. After two pregnancies with abruption, that risk rises to about 25%. Tell your doctor or midwife about your history so they can monitor you closely.
Smoking During Pregnancy
Smoking significantly raises the risk of placental abruption. The risk increases by about 20% for every 10 cigarettes smoked per day during pregnancy. Between 15% and 25% of all placental abruption cases are linked to cigarette smoking. Quitting smoking is one of the most effective ways to lower your risk. Your family doctor or a walk-in clinic can connect you with free smoking cessation programmes available in most provinces.
Cocaine Use
Using cocaine during pregnancy is strongly linked to placental abruption. Cocaine constricts blood vessels and reduces blood flow to the placenta. If you are struggling with substance use, speak with your doctor — support programmes are available across Canada without judgement.
Physical Injury to the Abdomen
A direct blow to the abdomen — such as from a car accident or a fall — can trigger placental abruption. Always wear your seatbelt properly during pregnancy, with the lap belt below your belly. Seek care immediately after any abdominal trauma.
Premature Rupture of Membranes
When the membranes (the amniotic sac) break more than 24 hours before labour begins, the risk of placental abruption rises. Research suggests this complication develops in about 3% to 5% of these cases.
Other Risk Factors
Several additional factors are associated with a higher risk of placental abruption. These include:
- A history of uterine problems, such as uterine fibroids (leiomyoma)
- Multiple previous pregnancies
- Carrying twins or multiples — placental abruption affects roughly 12 in 1,000 multiple pregnancies
- A previous caesarean section, which slightly raises the risk
- Being over age 35 — the rate rises from about 3 in 1,000 pregnant women aged 20–24 to 7 in 1,000 for those over 35
- Low folic acid (folate) levels, which may affect blood vessels and circulation in the placenta
In addition, taking prenatal vitamins containing at least 0.4 mg (400 mcg) of folic acid daily is recommended for all women who are pregnant or may become pregnant. This also helps prevent neural tube defects. Health Canada’s guidance on folic acid is a helpful resource for anyone planning a pregnancy.
Symptoms of Placental Abruption
Recognising the symptoms of placental abruption early can make a critical difference. Symptoms can range from mild to severe, and they may appear suddenly.
Common symptoms include:
- Vaginal bleeding — This can be light or heavy. The amount depends on where the placenta has separated and how long it takes for blood to pass through. In some cases, there may be no visible bleeding at all if blood is trapped behind the placenta.
- Uterine tenderness or pain — The abdomen may feel sore, tight, or painful to the touch.
- Signs of premature labour — These include regular contractions, lower back pain or pressure, abdominal cramping, and a uterus that feels hard and rigid.
Not every woman will have all of these symptoms. However, any vaginal bleeding during pregnancy should be taken seriously. Do not wait to see if it gets better on its own.
How Placental Abruption Is Diagnosed
Your healthcare provider will assess your symptoms, check your blood pressure, and monitor your baby’s heart rate. An ultrasound may be used to look at the placenta, though not all abruptions show up clearly on imaging. Therefore, doctors also rely heavily on your symptoms and physical examination.
Blood tests may be done to check for signs of blood loss or clotting problems. Your baby’s heart rate will be monitored continuously using a fetal heart rate monitor. In some cases, the diagnosis is only confirmed during or after delivery.
According to the Mayo Clinic’s overview of placental abruption, there is no medical treatment that can reattach the placenta. Instead, care focuses on managing complications and ensuring the safest outcome for both mother and baby.
Treatment Options in Canada
Treatment for placental abruption depends on how far along you are in your pregnancy and how severe the abruption is. Your healthcare team will guide you through the options based on your specific situation.
Mild Cases
If the abruption is minor and both you and your baby are stable, your doctor may recommend close monitoring in hospital. This may include bed rest, frequent fetal heart monitoring, and blood tests. In some cases, if you are less than 34 weeks pregnant, your doctor may give you corticosteroid injections to help the baby’s lungs develop faster.
More Severe Cases
If the abruption is significant, early delivery may be necessary to protect your life and your baby’s life. This might mean inducing labour or performing an emergency caesarean section. Blood transfusions may also be needed if there has been heavy blood loss. Your healthcare team will act quickly to manage any complications.
Most hospitals across Canada have obstetric emergency teams trained to handle placental abruption. If you give birth at a smaller regional hospital, you may be transferred to a larger centre with a neonatal intensive care unit (NICU) if your baby arrives early.
When to See a Doctor
If you experience any vaginal bleeding, sudden abdominal pain, or uterine tenderness during pregnancy, seek medical care right away. Do not wait for your next scheduled appointment.
In Canada, your options for urgent care include:
- Your family doctor — Call their office first if you are not sure whether your symptoms are urgent. Many clinics offer same-day appointments for pregnancy concerns.
- A walk-in clinic — A good option if your family doctor is unavailable and your symptoms are not severe.
- The emergency department — Go immediately if you have heavy bleeding, severe abdominal pain, or you are not feeling the baby move normally. Call 911 if needed.
In Canada, pregnancy-related emergency visits are covered under provincial health plans. You should never avoid seeking care due to cost concerns. If you do not have a family doctor, contact your provincial health authority — most provinces have a nurse hotline, such as 811, available 24 hours a day.
As always, speak with your healthcare provider about any concerns during your pregnancy. This article is for general information only and is not a substitute for professional medical advice. The World Health Organization highlights that fast access to skilled care is one of the most important factors in preventing serious pregnancy complications.
Frequently Asked Questions About Placental Abruption
What does placental abruption feel like?
Placental abruption often causes sudden abdominal pain, uterine tenderness, and vaginal bleeding. Some women describe the uterus feeling very hard or rigid. However, in some cases there is no visible bleeding, which is why any unusual pain during pregnancy should be assessed by a doctor right away.
Can placental abruption happen without bleeding?
Yes, placental abruption can occur without visible vaginal bleeding. This is called a concealed abruption, where blood collects behind the placenta instead of flowing out. In these cases, abdominal pain and uterine hardness are often the main warning signs.
What are the main causes of placental abruption?
The exact cause of placental abruption is not always known. However, the most common risk factors include high blood pressure, smoking, cocaine use, abdominal trauma, and a previous placental abruption. Managing these risk factors with your healthcare provider can help reduce your chances of developing this complication.
Is placental abruption life-threatening?
Placental abruption can be life-threatening for both the baby and the mother, especially in severe cases. It can cause heavy blood loss in the mother and oxygen deprivation in the baby. However, with fast medical treatment, most mothers and babies survive this complication successfully.
Can I have a healthy pregnancy after placental abruption?
Many women go on to have healthy pregnancies after experiencing placental abruption. Your risk of it happening again is higher, ranging from 4% to 17%, so your next pregnancy will be monitored more closely. Working with your doctor to manage risk factors — like blood pressure and smoking — greatly improves your chances of a healthy outcome.
How is placental abruption treated in Canada?
According to Mayo Clinic’s guide to placental abruption, this information is supported by current medical research.
For more information, read our guide on breast mastitis causes and treatment during pregnancy.
Treatment for placental abruption in Canada depends on the severity and how far along the pregnancy is. Mild cases may involve hospital monitoring and rest, while more severe cases may require early delivery by induced labour or caesarean section. Treatment is covered under provincial health insurance plans, so Canadians should always seek care without delay.
Key Takeaways
- Placental abruption occurs when the placenta separates from the uterine wall before birth, affecting about 9 in 1,000 pregnancies.
- It can cause serious complications including heavy bleeding, premature birth, and low birth weight.
- The most common risk factors include high blood pressure, smoking, cocaine use, and a history of previous abruption.
- Symptoms include vaginal bleeding, abdominal pain, and a hard or tender uterus — seek care immediately if these occur.
- There is no way to reattach the placenta; treatment focuses on monitoring and, when necessary, early delivery.
- In Canada, emergency pregnancy care is covered under provincial health plans — always call 811 or go to your nearest emergency department if you are concerned.
- Talk to your family doctor or midwife about your personal risk factors at your next prenatal visit.
Frequently Asked Questions
What is placental abruption?
Placental abruption is a serious pregnancy complication where the placenta partially or completely separates from the uterine wall before delivery. This disrupts oxygen and nutrient supply to the baby. It occurs in approximately 1% of pregnancies and requires immediate medical attention, as it can be life-threatening for both mother and baby.
What are the warning signs of placental abruption?
Common warning signs include sudden, severe abdominal or back pain, vaginal bleeding (though bleeding may be hidden internally), uterine rigidity or tenderness, frequent contractions, and reduced fetal movement. Symptoms can appear gradually or onset suddenly. Not all cases involve visible bleeding, making abdominal pain the most important warning sign.
When should I go to the hospital for placental abruption?
Go to the emergency room immediately if you experience sudden abdominal pain, vaginal bleeding, or notice your baby moving less than usual during pregnancy. Do not wait for a scheduled appointment. Placental abruption is a medical emergency — calling 911 or going directly to the nearest Canadian hospital is strongly recommended.
How is placental abruption treated in Canada?
Treatment depends on severity and gestational age. Mild cases may involve hospital monitoring and bed rest. Severe cases often require emergency delivery, either induced vaginally or by emergency C-section. Blood transfusions may be needed for significant blood loss. Canadian hospitals follow evidence-based protocols to protect both mother and baby.
Can placental abruption be prevented?
While placental abruption cannot always be prevented, you can reduce your risk by avoiding smoking, alcohol, and cocaine; controlling high blood pressure; wearing seatbelts properly during pregnancy; and attending all prenatal appointments. Women with prior abruption or clotting disorders should discuss preventive strategies with their Canadian healthcare provider.
About the Author
Dr. James Okafor, MD, PhDDr. James Okafor holds an MD and PhD in Neurological Sciences from McGill University. With 12 years of experience in clinical neurology and mental health research, he has contributed to landmark studies on depression, anxiety, and cognitive health. Dr. Okafor is a Fellow of the Royal College of Physicians and Surgeons of Canada and serves on the editorial board of two peer-reviewed journals.
View all articles →

{kind=link}