
Polycystic Kidney Disease: Symptoms & Care in Canada
Share
Polycystic kidney disease (PKD) is a genetic condition in which clusters of fluid-filled cysts develop inside the kidneys, gradually enlarging them and impairing their ability to function. It is one of the most common inherited kidney disorders affecting Canadians of all ages and ethnic backgrounds, and understanding the condition early can make a significant difference in long-term health outcomes.
Understanding Polycystic Kidney Disease and How It Develops
As PKD progresses, the growing cysts can cause a range of PKD symptoms Canada healthcare providers frequently assess, including chronic pain, high blood pressure, and blood in the urine. This article explains how polycystic kidney disease develops, what warning signs to watch for, how it is diagnosed in Canada, and what steps you can take to protect your kidney health.
What Is Polycystic Kidney Disease?
| Type | Characteristics | Age of Onset | Management Approach |
|---|---|---|---|
| Autosomal Dominant PKD (ADPKD) | Most common form; caused by mutations in PKD1 or PKD2 genes; cysts develop gradually in both kidneys; may also affect liver and cardiovascular system | Typically 30–50 years; symptoms may appear earlier | Blood pressure control, tolvaptan (Jynarque) for eligible patients, pain management, regular monitoring by a nephrologist |
| Autosomal Recessive PKD (ARPKD) | Rare and more severe form caused by PKHD1 gene mutation; affects kidneys and liver; enlarged kidneys detectable at birth or in utero | Infancy or early childhood; sometimes detected prenatally | Supportive care, management of hypertension, treatment of liver complications, dialysis or transplant in severe cases |
| Early-Stage PKD | Small cysts present; kidney function largely preserved; minimal or no symptoms; hypertension may begin to develop | Varies by type; often diagnosed incidentally via imaging | Lifestyle modifications, blood pressure management, increased fluid intake, annual kidney function monitoring |
| Advanced-Stage PKD | Significantly enlarged kidneys with numerous large cysts; declining GFR; increased risk of urinary tract infections, kidney stones, and cyst rupture | Typically 50–70 years in ADPKD | Nephrology specialist care, preparation for renal replacement therapy, dialysis, or kidney transplantation through a Canadian transplant program |
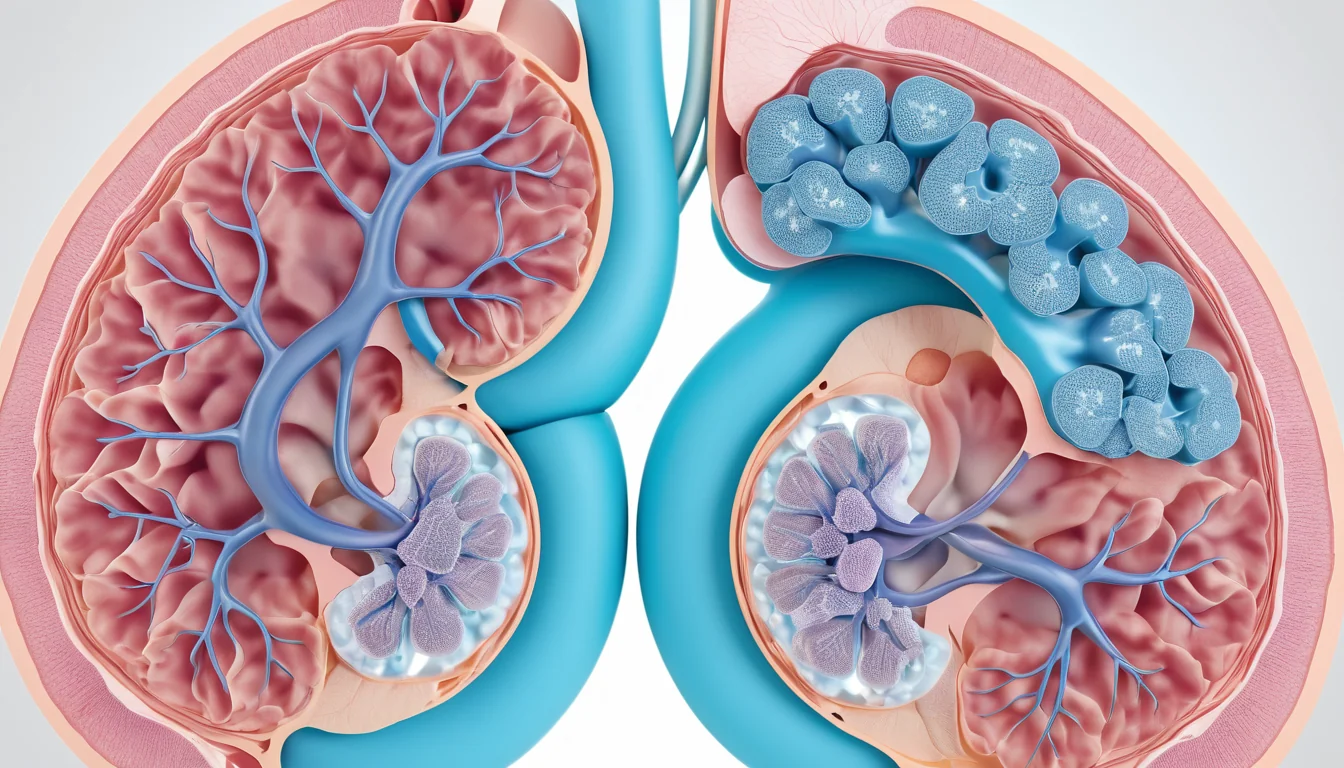
Healthy kidneys each weigh about 150 grams. In polycystic kidney disease, the kidneys can grow to weigh between 2,500 and 4,000 grams. That is more than 25 times the normal weight.
The cysts themselves are small, sac-like pockets filled with fluid. They can form anywhere along the kidney — in both the inner and outer layers of tissue. Cysts range in size from 0.1 cm to 10 cm or more.
Because ultrasound technology has improved so much, doctors are detecting kidney cysts earlier and more often than before. Many Canadians find out they have cysts during a routine checkup or imaging test done for another reason.
Types of Polycystic Kidney Disease
PKD comes in different forms. Each type affects the body in a slightly different way. Understanding the type you have helps guide treatment decisions.
Autosomal Dominant PKD (ADPKD)
This is the most common form of polycystic kidney disease in adults. You only need to inherit one copy of the changed gene from one parent to develop ADPKD. It affects not only the kidneys but also other organs, including the liver, pancreas, spleen, thyroid, and ovaries.
There are two subtypes. Type I involves a gene change on chromosome 16. Type II involves a gene change on chromosome 4. Type I tends to progress more quickly than Type II.
Autosomal Recessive PKD (ARPKD)
This rarer form usually appears in infants and young children. Both parents must carry the changed gene for a child to develop ARPKD. In this form, only the kidneys develop cysts — other organs are generally not affected.
Medullary Cystic Disease
In this type, cysts form only in the inner layer of the kidney, called the medulla. The outer layer, called the cortex, stays clear of cysts. This form is less common than the dominant type.
How Do Kidney Cysts Form?
Each kidney contains about one million tiny filtering units called nephrons. Every nephron includes a filtering ball (the glomerulus) and a system of tiny tubes that process waste and water.
In polycystic kidney disease, small outgrowths called diverticula form along these tubes. Over time, these outgrowths grow larger, break off, and close in on themselves. This creates a sealed cyst that traps tubular fluid inside.
The cells lining the cyst wall then begin to secrete more fluid. As a result, the cyst keeps growing. Even after a cyst is drained, the lining cells produce new fluid and the cyst can refill.
Symptoms of Polycystic Kidney Disease
Some people with polycystic kidney disease have no symptoms for many years. They may only discover the condition during a routine ultrasound. However, as cysts grow, symptoms usually appear.
Pain and Discomfort
Lower back or flank pain is the most common symptom of PKD. Chronic pain happens when growing cysts stretch the kidney’s outer lining and pull on surrounding structures. Sudden, sharp pain can occur when a cyst ruptures.
Pain intensity varies depending on the number, size, and location of the cysts. Draining a cyst — either surgically or through a needle — can reduce pain significantly.
Blood in the Urine
Blood in the urine (called haematuria) is common in PKD. It can be microscopic, meaning only visible under a microscope, or macroscopic, meaning visibly red or pink urine. Haematuria can result from a ruptured cyst, a cyst infection, bleeding inside a cyst, or kidney stones.
High Blood Pressure
High blood pressure (hypertension) is an early and very common complication of polycystic kidney disease. It often develops before any loss of kidney function. Cysts pressing on kidney tissue reduce blood flow, which signals the body to raise blood pressure through a hormone called renin.
Uncontrolled high blood pressure is dangerous. Over time, it can damage the heart, blood vessels, and brain. It is one of the leading causes of serious illness and death in people with PKD. Managing blood pressure is a key part of treatment.
Kidney Infections and Kidney Stones
Infected cysts cause fever and pain in the side or back. Infections and other metabolic changes also create conditions that lead to kidney stones. In fact, about 30% of people with PKD develop kidney stones. These stones are often made of uric acid or oxalate crystals.
Complications Beyond the Kidneys
Polycystic kidney disease does not stay confined to the kidneys. In the autosomal dominant form, cysts and other problems can develop in several other parts of the body.
Liver Cysts
Liver cysts are the most common non-kidney complication of ADPKD. About one-third of people with PKD develop them. Liver cysts appear later in life than kidney cysts. They do not usually affect liver function. However, they can cause discomfort, pain, or difficulty breathing if they grow very large. In those cases, a doctor may drain them.
Research suggests that the number of liver cysts in women may be linked to the number of pregnancies they have had. Furthermore, all people with ADPKD will eventually develop some liver cysts.
Cysts in Other Organs
About 10% of people with PKD develop pancreatic cysts. About 5% develop cysts on the spleen. These cysts rarely cause symptoms but are worth monitoring.
Brain Aneurysms
People with polycystic kidney disease have a higher-than-average risk of developing an intracranial aneurysm. This is a bulge in a blood vessel in the brain that can rupture and cause a stroke. Doctors can detect aneurysms using a CT scan or MRI. If you have a family history of brain aneurysms along with PKD, tell your doctor right away.
How Is Polycystic Kidney Disease Diagnosed?
Doctors use several tools to diagnose polycystic kidney disease and track its progression.
Ultrasound
Ultrasound is the first-choice imaging test for PKD. It is safe, affordable, widely available at imaging centres across Canada, and does not use radiation. Ultrasound can detect cysts larger than 0.5 cm. Most provincial health plans cover diagnostic ultrasounds when ordered by a physician.
Urine Tests
Urine tests look for blood (haematuria), protein (proteinuria), and the kidney’s ability to concentrate urine. Protein in the urine is a sign of kidney stress. In PKD, protein levels are usually low — under 1 gram per day — and come from the tubular cells rather than the filtering units. A reduced ability to concentrate urine appears in later stages of the disease.
Blood Tests
Blood tests measure waste products like urea and creatinine. Rising levels of these substances indicate that the kidneys are losing their filtering ability. In PKD, there is an interesting pattern: anaemia is often milder than expected, even when creatinine levels are quite high. This is different from other forms of chronic kidney disease.
CT Scan and MRI
CT scans and MRI provide more detailed images than ultrasound. They are especially useful for detecting brain aneurysms or mapping cysts in complex cases. Your family doctor can refer you for these tests through the provincial health system.
Kidney Function Over Time
For many years, kidney function can remain completely normal in people with polycystic kidney disease. However, around age 40, kidney function typically begins to decline. Without treatment and monitoring, this can progress to kidney failure (also called end-stage renal disease) within about 10 years.
When the kidneys can no longer filter waste effectively, patients need dialysis or a kidney transplant to survive. In Canada, dialysis is available through provincial health programmes at hospital centres and satellite clinics. Health Canada provides resources on kidney disease support programmes available in each province.
Therefore, early diagnosis and ongoing monitoring are essential. Regular checkups with your family doctor help catch changes in kidney function before they become a crisis.
When to See a Doctor
You should see your family doctor if you notice any of the following: blood in your urine, persistent lower back or side pain, a lump or fullness in your abdomen, frequent urinary tract infections, or high blood pressure that is hard to control.
If you have a parent or sibling with polycystic kidney disease, ask your family doctor about genetic screening. PKD runs in families, so early testing can help you and your doctor plan ahead. If you do not have a family doctor, a walk-in clinic can assess your symptoms and arrange an ultrasound referral.
For more information on kidney health, visit the Mayo Clinic’s guide to polycystic kidney disease or review resources from the World Health Organization on chronic kidney disease.
Always speak with a qualified healthcare provider before making any decisions about your health or treatment. This article is for general information only and does not replace medical advice.
What is polycystic kidney disease and is it serious?
Polycystic kidney disease is a genetic condition where fluid-filled cysts grow in the kidneys, causing them to enlarge and lose function over time. It is a serious condition because it can lead to high blood pressure, kidney failure, and complications in other organs. However, with early diagnosis and proper management, many people with PKD live full and active lives.
Is polycystic kidney disease hereditary?
Yes, polycystic kidney disease is a hereditary condition passed down through families. The most common form, autosomal dominant PKD, means that a child has a 50% chance of inheriting it if one parent carries the gene. If PKD runs in your family, ask your family doctor about genetic testing and screening.
What are the first signs of polycystic kidney disease?
The first signs of polycystic kidney disease often include high blood pressure, lower back or flank pain, and blood in the urine. Some people have no symptoms at all and are only diagnosed during a routine ultrasound. Because symptoms can be mild at first, regular checkups with your family doctor are important if you have a family history of PKD.
Can polycystic kidney disease be cured?
There is currently no cure for polycystic kidney disease, but treatments can slow its progression and manage symptoms. A medication called tolvaptan is approved in Canada to slow cyst growth in certain adults with ADPKD. Controlling blood pressure, staying hydrated, and maintaining a healthy lifestyle also play an important role in protecting kidney function.
Does polycystic kidney disease always lead to dialysis?
Not everyone with polycystic kidney disease will need dialysis, but the risk is significant. About half of people with ADPKD develop kidney failure by age 60 and require dialysis or a kidney transplant. Early detection and consistent management of blood pressure and other risk factors can delay this outcome for many years.
How is polycystic kidney disease diagnosed in Canada?
According to Mayo Clinic’s overview of polycystic kidney disease, this information is supported by current medical research.
For more information, read our guide on warning signs of kidney disease in Canada.
In Canada, polycystic kidney disease is most commonly diagnosed using an abdominal ultrasound, which is covered by most provincial health plans when ordered by a doctor. Your family doctor may also order urine tests, blood tests, or a referral for an MRI or CT scan. Genetic testing is available through specialist referrals for those with a strong family history of PKD.
Key Takeaways
- Polycystic kidney disease is a genetic condition causing fluid-filled cysts to grow in the kidneys and sometimes other organs.
- The most common form, ADPKD, affects adults and can be passed from parent to child with a 50% chance per pregnancy.
- High blood pressure is an early and serious complication that requires prompt management.
- Common symptoms include back pain, blood in the urine, and frequent infections.
- Kidney function can remain normal for decades, but decline often begins around age 40.
- Ultrasound is the safest and most widely used diagnostic tool, covered by most provincial health plans.
- About 30% of PKD patients develop kidney stones, and all ADPKD patients eventually develop liver cysts.
- Brain aneurysms are a rare but serious risk — mention any family history to your doctor.
- If you have symptoms or a family history of PKD, see your family doctor or visit a walk-in clinic for an assessment.
Frequently Asked Questions
What is polycystic kidney disease?
Polycystic kidney disease (PKD) is a genetic disorder where clusters of fluid-filled cysts develop in the kidneys, causing them to enlarge and gradually lose function. It is one of the most common inherited kidney conditions in Canada, affecting approximately 1 in 500 people and potentially leading to kidney failure if untreated.
What are the symptoms of polycystic kidney disease?
Common symptoms of polycystic kidney disease include high blood pressure, back or side pain, blood in the urine, frequent kidney infections, a feeling of fullness in the abdomen, and headaches. Some people experience no symptoms for years, as PKD often progresses slowly before causing noticeable problems.
How is polycystic kidney disease treated in Canada?
Treatment focuses on managing symptoms and slowing progression. Canadian doctors may recommend blood pressure medications, pain management, antibiotics for infections, and lifestyle changes. Tolvaptan (Jynarque) is an approved medication in Canada that can slow cyst growth. Advanced cases may require dialysis or a kidney transplant.
Can polycystic kidney disease be prevented?
PKD cannot be prevented as it is primarily genetic. However, progression can be slowed by controlling blood pressure, staying well hydrated, following a low-sodium diet, avoiding smoking, maintaining a healthy weight, and limiting caffeine. Genetic counselling is recommended for Canadians with a family history of PKD.
When should you see a doctor about kidney cysts or PKD symptoms?
See a doctor promptly if you experience persistent back or side pain, blood in your urine, recurring urinary tract infections, or high blood pressure. Canadians with a family history of PKD should request screening even without symptoms. Sudden severe headache or chest pain requires immediate emergency care.
About the Author
Dr. James Okafor, MD, PhDDr. James Okafor holds an MD and PhD in Neurological Sciences from McGill University. With 12 years of experience in clinical neurology and mental health research, he has contributed to landmark studies on depression, anxiety, and cognitive health. Dr. Okafor is a Fellow of the Royal College of Physicians and Surgeons of Canada and serves on the editorial board of two peer-reviewed journals.
View all articles →

{kind=link}